By Frederick de Sam Lazaro
A couple of years ago, I was returning from reporting on AIDS in South Africa and decided that we’d make a side trip to Rwanda. I had learned early the lesson that there are no “side trips” to neighboring countries in Africa. Fortunately, in this case, we found a connection that would have us spend just one night in Nairobi. Flying up on Kenya Airways, I noticed in the airline magazine that you didn’t need a visa to be in Kenya for fewer than 30 days.
Well, we got to the Nairobi airport and, sure enough, the immigration officer said to me, “You need a visa, go to the visa counter.” So I walked over to the visa counter and there, bold-faced, was a sign that indicated I didn’t need a visa. So I said to the gentleman at the counter, “What’s the deal? The airline magazine says that I don’t need a visa, and the sign here says I don’t need a visa. Why are you charging us for visas?” He said to me the words that have stuck with me ever since. “Oh, that sign,” he said, “that has been a very troubling sign. It has been giving us all kinds of trouble for many, many, many days!” He said, “It is a very shallow sign. It is an extremely shallow sign.”
You really live for moments like that on the road. I’ve often reflected on that phrase, “the shallow sign,” and I wonder if my Kenyan friend might not think that some of the stories that we do on television are the shallow signs of what’s going on. When talking about AIDS in Africa, India, and Thailand, there’s just such an enormous amount of information. So I want to suggest just three “deeper” signs that might inform the trajectory of infection rates and indicate how the AIDS epidemic is going to progress.
First of all, it boils down to what the political or societal leadership is doing or saying about AIDS. And by societal leadership I mean people who have clout: movie stars in countries like India — what are they saying or doing about AIDS, do they think it’s a priority? Second, what are the conditions in which women live in that country: their health status, their economic status, their “human-rights status?” And a somewhat distant third: What is the attitude of the religious leadership in this country? There may even be a fourth, and that’s plain luck. There’s no really good reason why Thailand has a raging epidemic, for example, and the Philippines doesn’t. Why India has so many cases and Bangladesh doesn’t.
Let’s begin with South Africa. For someone like me, sitting in Minneapolis and trying to cover international stories, I need a certain amount of a “buzz” to get the assignment. Is Mike Wallace doing this story? Is The New York Times writing about it? And there was precious little buzz about AIDS in Africa for much of the ’90s until it started to be an epidemic in South Africa, a nation that we as Americans have for various reasons followed much more closely, with its fabled transformation to democracy under Mandela. Yet throughout his presidency, Nelson Mandela never uttered a word in public about HIV or AIDS, even as his country was developing what by the end of his tenure was the largest epidemic in the world, close to four million infections in a country of 40 million. This, despite having the most sophisticated media, as well as health-surveillance system, on the continent.
Now, off to the east in Africa there was a warlord named Yoweri Museveni who took power in Uganda in the mid ’80s with little to distinguish himself from Milton Obote and Idi Amin, the despots who preceded him. Yet Museveni did one thing that was unheard of until then in newly-independent Africa: He declared that Uganda had a problem and that anybody in the world who had ideas was welcome to come and help. In sharp contrast, Uganda’s neighbor, Kenya, deathly afraid that safari tourists would stay away, denied that it had any problems with AIDS.
Museveni’s exhortation sparked some of the most creative and imaginative public-health initiatives until then and perhaps since. There were AIDS service organizations that provided support for people who were HIV positive. There were dance groups tailored to send the message of prevention to the 31 different tribes and cultures in Uganda. Music stars helped to further de-stigmatize the disease, and the Islamic Association sent out middle-aged women to teach young women how to use condoms. I remember vividly something that a woman who started the AIDS service organization of Uganda said. “If I can live until my daughter is 16 instead of eight, then I will have raised a much more viable orphan.” Today, Uganda’s infection rate has dropped from 14 percent of the adult population to 8 percent. Kenya, meanwhile, has seen its infection rate climb to 15 percent of the adult population. And in South Africa, one out of five adults today is HIV positive.
Then you go west to Senegal, where the rate has consistently stayed below 2 percent. This is a country that has many of the same raw ingredients for an epidemic: a maritime-based regional economic hub, a thriving commercial-sex industry, a tolerant society by the standards of Islam. What Senegal had, since the late ’60s, was a system of surveillance initially targeting sexually-transmitted diseases. Prostitution is legal in Senegal. Sex workers need to register themselves and are required to be tested monthly. There’s reasonable condom availability and usage.
A lot of things are credited for Senegal’s success, including the surveillance system that now watches for this virus. But, importantly, they afford a certain measure of protection to the women in Senegal. It is one of the happiest stories on the continent.
“If I can live until my daughter is 16 instead of eight, then I will have raised a much more viable orphan.”It’s a very different story in India, where four million people are infected, second only to South Africa. You talk to any number of people, and they tell you the actual infection rate is two to two-and-a-half times that number conservatively. No one disagrees that India will probably overtake sub-Saharan Africa in the next decade or so, which will mean more than 35 million infections. The Victorian sexual mores that prevent public discussion of sex or sexuality, insipid public-health campaigns, bureaucracy, and a deep-rooted caste system that writes off AIDS as a disease of people on the margins of society — these all lead to staggering numbers.
It’s an irony that this is a country with one of the most productive pharmaceutical industries in the world. Until now there hasn’t been a peep from top government officials on the issue of AIDS. And in the even more influential Bollywood movie industry, there has not been a Rock Hudson or Freddy Mercury figure who’s come out, even though several stars have been afflicted.
Perhaps most telling about India’s epidemic is the status of women. The most compelling measure may be that there are about five million sex-selective abortions in India each year. These are abortions by parents who have used ultrasonic scans to determine the sex of their fetus and aborted after discovering it was female.
Finally, to a more encouraging story — the poster-child country in the developing world — and that’s Thailand. This is a country that had one of the first epidemics in the developing world, centered around the thriving commercial-sex industry in Bangkok, which draws its workers from all parts of Thailand and from neighboring countries. Thailand had in place a condom campaign that is nothing short of breathtaking, and it began as a family-planning campaign in which they managed to de-stigmatize contraception, condoms in particular. It’s the only country I know in the world that has a condom-blowing contest on television. Now Thailand has seen the infection rate rise, especially among the young, because there were cutbacks in AIDS support after the Asian financial crisis. There’s a renewed effort to come up with a message that clicks with the emerging younger generation, not unlike what we’re seeing in the gay, white male population in the United States, which has also seen an increase in infection rates.
It’s the only country I know in the world that has a condom-blowing contest on television. Thailand’s challenge now is to care for one million people who are HIV positive, many of whom are now converting to AIDS. What is astonishing is that despite its reputation for tolerance, this is a nation where people don’t want to touch those with AIDS, and they are being cast out of family and village, with few places to go. The Buddhist monks have opened monasteries to accommodate people with AIDS in reasonable comfort. There are a very limited number of painkillers administered to people, but they at least can die in a bed. Most will not be visited by any family members. They die and are taken straight to a crematory, which is right on the premises, and the ashes of thousands are piled high. Every single day they have three to four deaths; one monastery has a waiting list of 10,000 people. All of a sudden you discover that a country that knows so much about AIDS has compassion in short supply.
A very personal note: I get uneasy talking to people who can’t tell me not to take their pictures or who can’t protest. At one AIDS hospice I visited, in a Buddhist monastery, thousands of tourists come through; it’s completely open. People are there in various stages of death, and one can just go in and take pictures. I found it just completely unnerving. But the thing that really astonished me is how receptive the AIDS patients were to visitors. How can somebody whose small private space is being violated be so receptive to tourists and school kids asking silly questions? It struck me at that point that this may be where the compassion gap manifests itself, because these are people who have not had warm human contact ever since they became visibly symptomatic.
Thailand plans to make available the dollar-a-day antiretroviral cocktail drugs, which are going to greatly help reduce demand for facilities like these. The thing that boggles the mind as you look at that pile of ashes is how much life has been lost. Had these folks won the lottery and lived in the United States, they would be thriving human beings for several more years.
Frederick de Sam Lazaro is a correspondent for PBS’s NewsHour with Jim Lehrer and an executive producer at Twin Cities Public Television, in St. Paul. This article originally appeared in the Fall 2002 Journal of the Knight-Wallace Fellows.
Beyond Shallow Signs
More News

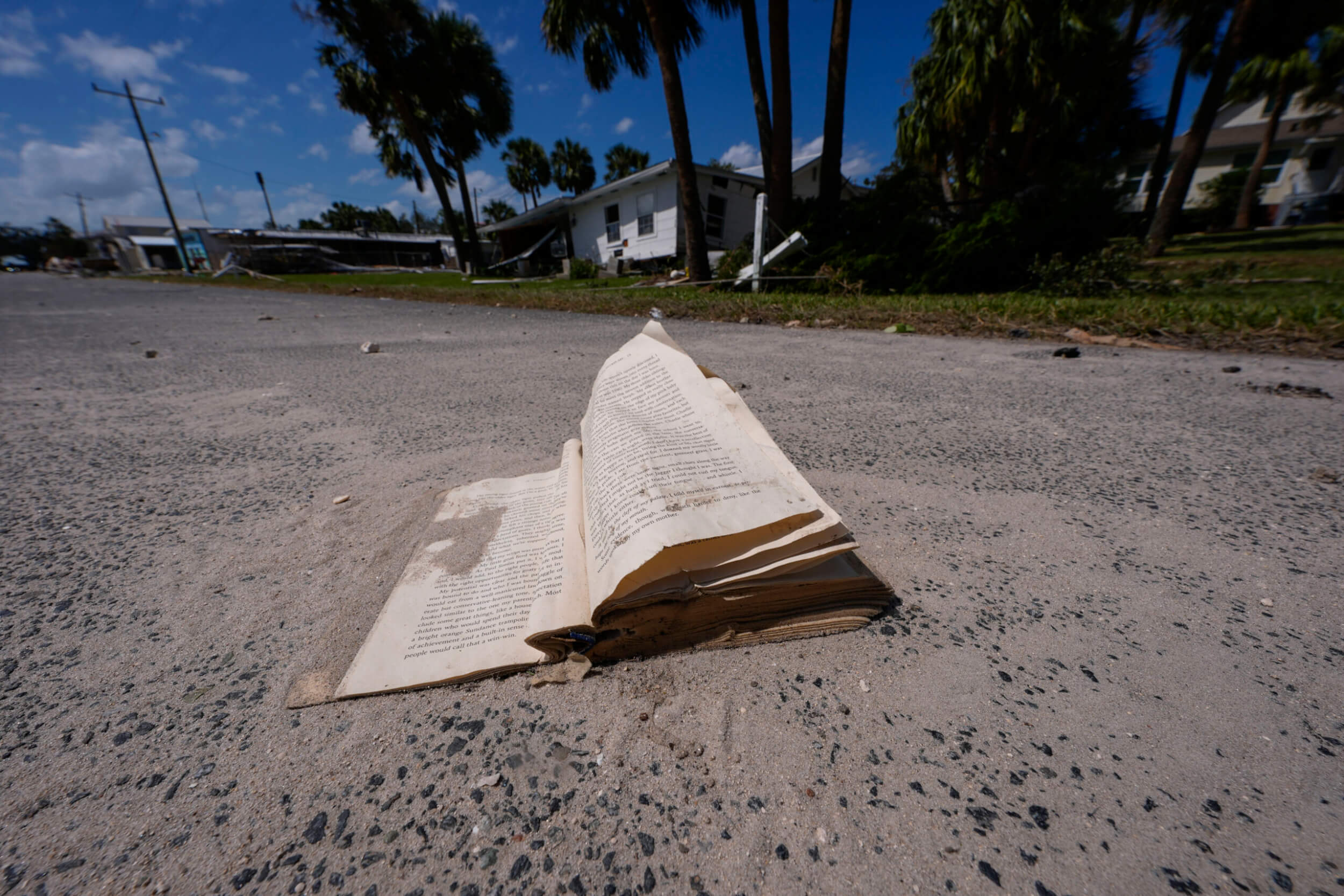
A photojournalist reported on dozens of hurricanes over the years. Then Hurricane Helene flooded his home.
Douglas R. Clifford was in Tallahassee, preparing to cover Helene for the Tampa Bay Times, when the storm came knocking at his door.
October 2, 2024
After Hurricane Helene, ‘Neighbors are what’s getting us through this’
Coverage and help from Florida and North Carolina
October 2, 2024

Opinion | Donald Trump to skip ‘60 Minutes’ interview
Appearing on ‘60 Minutes’ has become something of a tradition in American presidential politics. But Trump changed course and will not participate.
October 2, 2024

Fact check: What JD Vance and Tim Walz got right and wrong on abortion and immigration at the VP debate
Vance and Walz met in an Oct. 1 vice presidential debate hosted by CBS News that was cordial and heavy on policy discussion
October 2, 2024

Opinion | International news is on the line in the upcoming presidential election
There’s always a downturn in international giving during election season, and the future of that giving depends largely on who is elected
October 2, 2024