Covering COVID-19 is a daily Poynter briefing of story ideas about the coronavirus and other timely topics for journalists, written by senior faculty Al Tompkins. Sign up here to have it delivered to your inbox every weekday morning.
Covering COVID-19 is a daily Poynter briefing of story ideas about the coronavirus and other timely topics for journalists, written by senior faculty Al Tompkins. Sign up here to have it delivered to your inbox every weekday morning.
Think it is hard to get people to wear a mask? Wait until health workers try to vaccinate the entire population.
A recent survey conducted by the Pew Research Center found that if a COVID-19 vaccine were available today and proven effective, only 54% of Black adults would be willing to get it, compared to 74% of white adults.
The findings reflect a distrust among Black Americans toward the health care industry generally and medical research specifically. The Pew survey found:
35% of black Americans have a great deal of confidence in medical scientists to act in the public interest, compared with 43% of white adults.
Similar patterns appear on other questions, too.
Around half of black Americans (53%) have a mostly positive view of medical research scientists, compared with around two-thirds of Hispanic (67%) and white adults (68%).
Around six-in-ten black adults (61%) have a mostly positive view of medical doctors, versus 75% of white adults.
The idea that people are not enamored with new vaccines is steeped in history. When the polio vaccine came out to great fanfare in 1955, the program had to be quickly abandoned because the vaccine itself caused 40,000 cases of polio, killing 10 and leaving 200 children with varying degrees of paralysis. It was a disaster. That incident led to a process now in place to ensure vaccines are safe and effective before they hit the market.
Heck, even now 43% of American adults don’t get the flu vaccine even though 80,000 Americans died from the flu last year. About a fourth of those who passed up a flu shot said they just didn’t think they would get sick.
When I was a little guy, I remember seeing pictures like this. It was called an “iron lung” and it was a machine in which polio patients lived, sometimes for months or even years.

This historic 1960 photograph depicted a nurse caring for a victim of a Rhode Island polio epidemic, who was inside an Emerson respirator, also sometimes referred to as an iron lung machine. (From the Centers for Disease Control and Prevention photo archive)
I remember people saying that if you didn’t get the polio vaccine you would end up in an iron lung. I clearly remember lining up at a school and popping a sugar cube that had some vaccine drops on it into my mouth. The government’s campaign worked on me. In the 1950s, the threat of getting polio was second only to being killed by an atomic bomb as “top worries.”
Dr. Lauren Grossman, an emergency room physician, wrote that we should consider making vaccinations mandatory. If the difficulty of getting people to wear a mask teaches us anything, it’s that Americans are suspicious and stubborn and don’t want to be told what to do. But the government has forced vaccinations before:
A 1905 Supreme Court decision established the constitutionality of compulsory state vaccination laws to protect the public health. Although all 50 states and the District of Columbia now require diphtheria, tetanus, pertussis, polio, measles, rubella, and varicella vaccinations before attending public school, all also offer a variety of vaccine exemptions for medical, religious, and philosophical reasons. Only 11 states can override these exemptions in an outbreak. Court decisions, including from the Supreme Court, have upheld both state-imposed fines for refusing to be vaccinated and the exclusion of unvaccinated children from schools.
Grossman, who is also an assistant professor of emergency medicine at the University of Colorado School of Medicine and medical director of the university’s Integrative Medicine Center, had several other suggestions for how to get vaccines out there fast once they are ready. For one thing, health insurance companies could tell their customers that they have to get vaccinated if they want coverage when they get sick. There are other ideas:
- Combine the coronavirus vaccine with another one (like influenza) and package them in a form that patients can take on their own.
- Allow it to be administered to individuals with low-grade symptoms. Tetanus immunization has been wildly successful in part because we administer the vaccination when someone is being seen for a wound, not weeks later when it has healed.
- Make coronavirus vaccination available in all health care facilities, physicians’ offices (no matter what the specialty), local health departments, and emergency or urgent care facilities. Make it clear that any physician or advanced practice provider can administer a vaccine.
- Offer vaccinations in workplaces, schools, pharmacies, and community organizations. That could mean visits from mobile teams (perhaps run by medical school students as part of their public health training) to provide immunizations.
- Make vaccinations inexpensive. Instead of costing as much as $70, the price tag for a high-dose influenza vaccination for seniors, the cost of a coronavirus vaccine should be affordable for all. Stores like Walmart, with its $4 medication list, could add immunizations and offer them as people come in to pick up their prescriptions.
Let’s not wait until there is a vaccine to start asking questions about what the government is doing to distribute it to hundreds of millions of people in a short period of time. The education effort required to pull this off will be monumental.
New polling shows the public is confused
The Pew Research Center’s new poll shows two-thirds of the public think the Centers for Disease Control and Prevention gets information about COVID-19 right, and close to a third think President Donald Trump and his administration get the facts right. Take that in for a second. Only a third of the American public believes the president gets basic facts right about the pandemic.
The implications of that are profound. What hope do we have that people will get inoculated if there is not more agreement on the basic facts about the virus?
Let’s dive into the Pew data to see what it says about where your reporting is most needed to help the public get clarity.
(Data and graphic from the Pew Research Center)
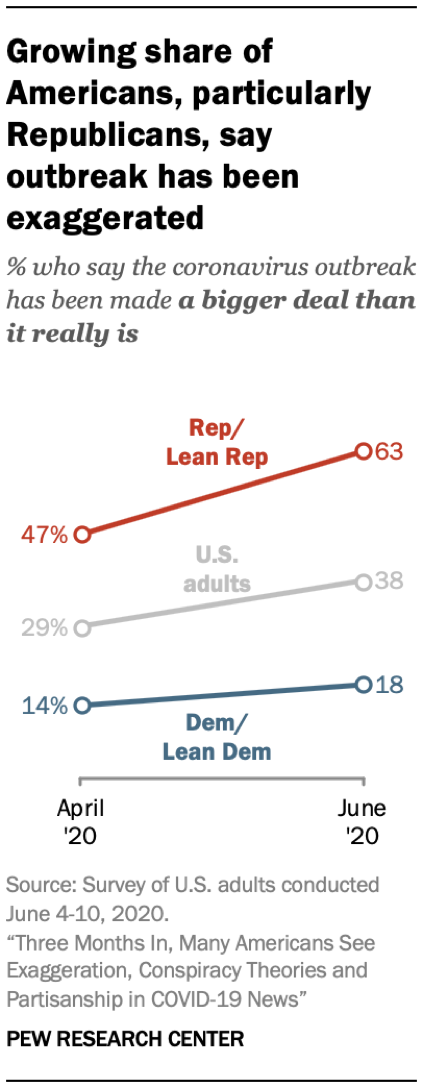
The survey shows that conversations about COVID-19 are increasingly partisan, and not as focused on medicine and science as they were a few months ago. Pew reports:
Compared with the first weeks of the outbreak, Americans report seeing more partisan viewpoints in news about COVID-19, and some are struggling to know what is true. About four-in-ten U.S. adults (41%) say news about the outbreak is now more partisan than at the start, while fewer say partisanship in coronavirus news has declined (22%). A plurality of U.S. adults (38%) say they now find it harder to identify “what is true and what is false about the outbreak,” while three-in-ten say they are finding this easier to do. Another 31% say the difficulty of parsing truth from fiction has not changed.
(Data and graphic from the Pew Research Center)
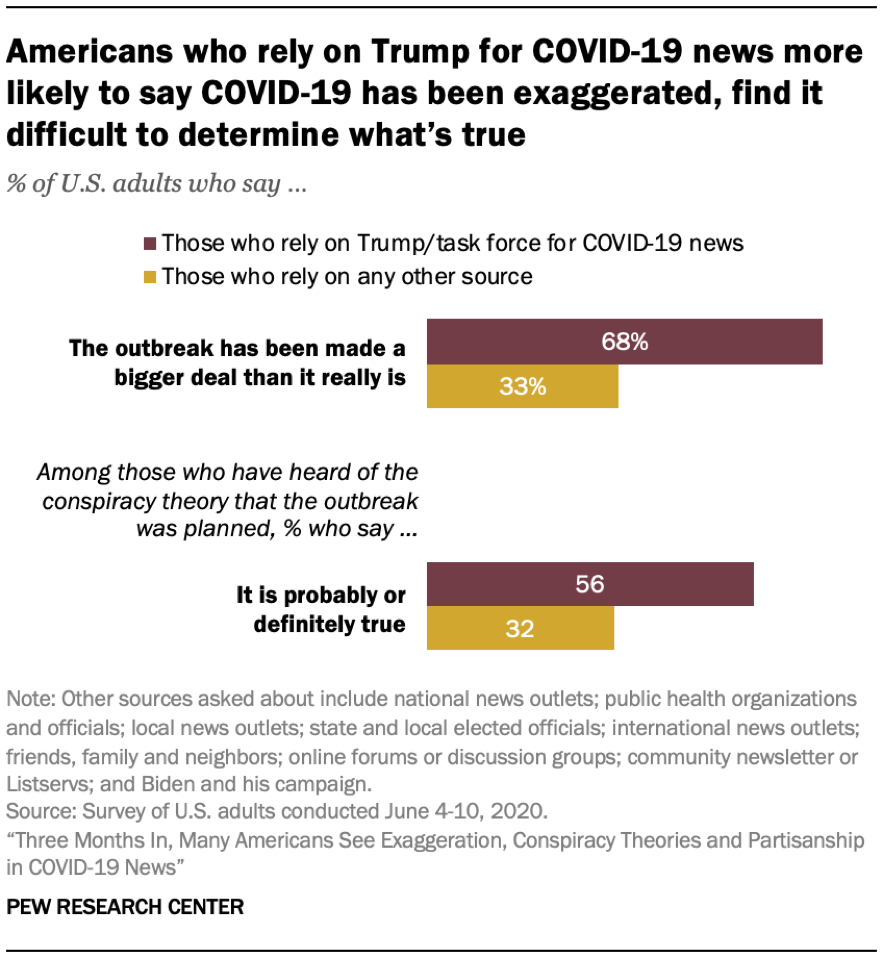
My Poynter colleagues at PolitiFact, MediaWise and the International Fact-Checking Network have documented and debunked hundreds of conspiracy theories, fakes and outright lies about COVID-19. But the one that seems to live on is the one about it all being a big plan:
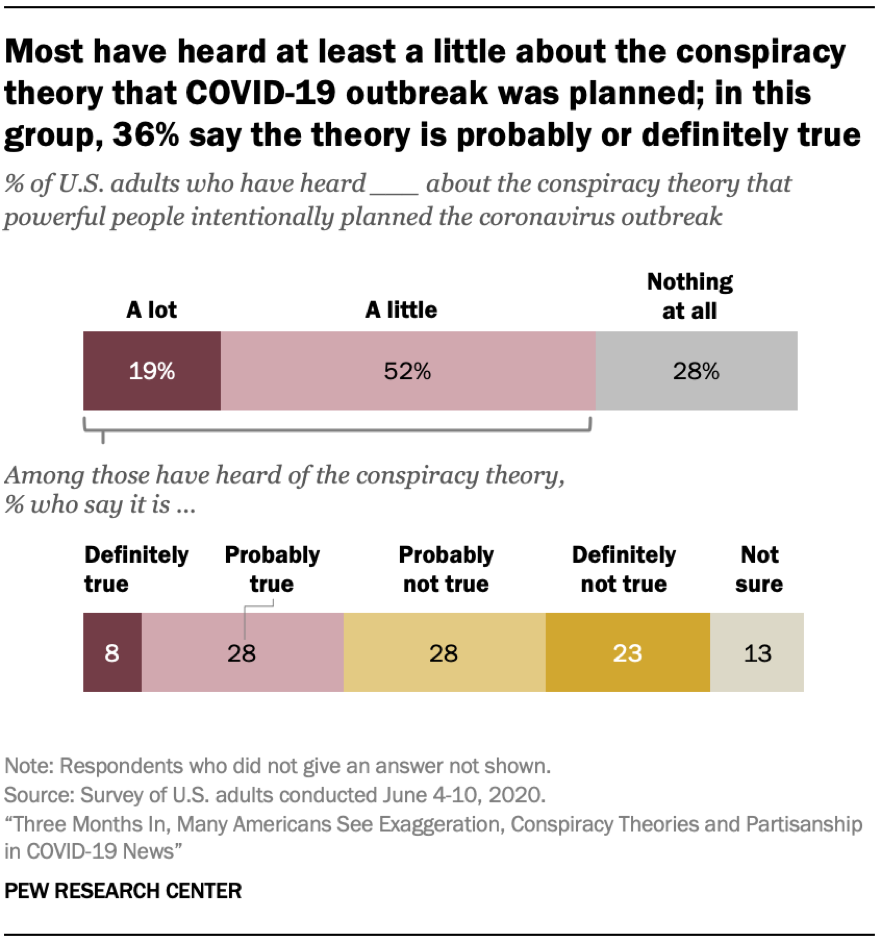
(Data and graphic from the Pew Research Center)
I pass that data along with caution: Just acknowledging a conspiracy gives it oxygen and new life.
[the_ad id=”667826″]
The COVID-19 drug that will cost more than $3,000
The Wall Street Journal reported:
Gilead Sciences Inc. detailed its pricing plans for Covid-19 drug remdesivir, saying it will charge U.S. hospitals $3,120 for a typical patient.
The drugmaker on Monday disclosed its pricing plans as it prepares to begin charging for the drug in July. The U.S. has been distributing remdesivir donated by Gilead since the drug was authorized for emergency use in May.
But the cost of the drug depends on who is paying for it. CNBC reported:
The drugmaker said it will sell Remdesivir for $390 per vial to governments “of developed countries” around the world, and the price for U.S. private insurance companies will stand at $520 per vial. In the U.S., that means Gilead will charge a lower price for government programs like Medicare and a higher price for private insurers.
The White House said since the drug is administrated while the patient is “in hospital,” a patient covered by insurance would not notice the price. Gilead said remdesivir would save $12,000 per patient by getting them out of the hospital faster.
This is an opportunity for journalists to explain how the price of drugs is never set in stone. It is always negotiable depending on who is buying it, who is using it, and whether they are privately insured or covered by government plans including Medicare and Veterans Affairs.
The CDC updated its COVID-19 symptoms with three additions
Can you spot the three new symptoms that the CDC added to its official COVID-19 list?
- Fever or chills
- Cough
- Shortness of breath or difficulty breathing
- Fatigue
- Muscle or body aches
- Headache
- New loss of taste or smell
- Sore throat
- Congestion or runny nose
- Nausea or vomiting
- Diarrhea
The list added congestion or runny nose, nausea or vomiting and diarrhea. The CDC said, “People with COVID-19 have had a wide range of symptoms reported — ranging from mild symptoms to severe illness. Symptoms may appear 2-14 days after exposure to the virus.”
The addition of these common afflictions will no doubt add to the number of people who go get checked for COVID-19.
The list is constantly evolving. Can you name the original three symptoms?
The first three were fever, cough, and shortness of breath or difficulty breathing.
[the_ad id=”667872″]
The surge of COVID-19 cases among Latinos
You have reported how Black Americans have been sickened by the coronavirus at far higher rates than other Americans, but the newest spike in COVID-19 cases is in counties where Latinos live in high concentrations. An analysis from The New York Times found:
… in the last two weeks, counties across the country where at least a quarter of the population is Latino have recorded an increase of 32 percent in new cases, compared to a 15 percent increase for all other counties, a Times analysis shows.
The CDC estimated “Hispanic or Latino persons have a rate approximately 4 times that of non-Hispanic white persons.” The CDC said this is not unusual, and that “history shows that severe illness and death rates tend to be higher for racial and ethnic minority populations during public health emergencies than for other populations.” Since we know that to be true, it’s worth exploring how the government is dispensing resources to test and help care for that sector of the population.
The rates are two times higher in 30 states, and over four times higher in eight states. For example, in Virginia more than 12,000 cases — 49% of all cases with known ethnicity — come from the Hispanic and Latino community, which makes up only 10% of the population.
It is important to point out that there is no reason to believe that any race or ethnicity is more vulnerable than another to the virus. The spread among Latinos may mostly be reflective of the fact that Latinos make up a lot of what we consider to be “essential workers,” and as such are more exposed to the virus because they cannot stay home.
Latinos are dying at a lower rate than other ethnicities, however, partly because nearly three-quarters are millennials or younger, according to data from the Pew Research Center. Younger COVID-19 patients are less likely to die than older people.
Another issue you probably have not heard about is whether drug trials will include a representative sample of people. Usually, drug trials skew heavily white. Stat reported:
In 2019, for example, the Food and Drug Administration approved 11 new cancer drugs based on clinical trials that enrolled just 4% of Black participants, despite the fact that Black individuals account for 13% of the U.S. population and have the highest death rate for most cancers.
To be demographically representative of the U.S. population, drug trials would need about 40% of the participants to be non-white. The Stat article pointed out other barriers:
The hours that clinics are open are too limited for people of color whose employers prohibit taking off work; study budgets don’t always pay for interpreters and translations that would facilitate participation by non-English speakers; study protocols often exclude individuals with chronic illnesses like diabetes and hypertension, which disproportionately impact people of color.
Who is caring for the office plants while you are away?
The New York Times produced a fun piece on the office plant care business that is trying to keep your greenery alive while you are gone. It turns out that with lights off and air handlers turned way down the plants are growing slower.
How did COVID-19 cause a coin shortage?
The economic slowdown caused by COVID-19 created a national shortage of coins, just one more interruption to our lives.
Federal Reserve Chair Jerome Powell said, “We are working with the Mint and the Reserve Banks and as the economy reopens we are starting to see money move around again.”
The shortage is significant enough that the federal government started limiting how many pennies, nickels, dimes and quarters it sends to banks. Businesses say they would love it if you could give them exact change for your purchase, or better yet, pay with a bunch of coins.
(Screenshot, Facebook)
The Fed suggested that banks loosen their regulations on accepting loose and rolled coins, which have become a pain in the behind over the years. I remember a day when you could take a jar of coins to a bank, dump them in a machine and they would give you dollar bills back. Now you either wrap them yourself and put a bank deposit number on every roll or you take them to a machine at the grocery and pay a percentage just to have the machine count the money.
I also wonder how long it will take for the U.S. to do what Canada did, which I do not like. Canadians got rid of the penny and started rounding prices. This is the way the National Canadian Mint explained it:
If the purchase end with .01 or .02 or it ends with .06 or .07 you round it down to .00 or .05, you are rounding to the closet nickel.
If it ends with .03 or .04 or it ends with .08 or .09 you round up or the closest nickel.

(National Canadian Mint)
I teach a fair amount in Canada and I am always annoyed when I find that everything I buy seems to magically end in a “round-up” number. These are the examples the Mint gives:

(National Canadian Mint)
So you round up to $1.90. By the way, that $1.80 will only get you a medium Tim Hortons coffee. Just saying.

(National Canadian Mint)
Let me tell you, you are not going to find that big honking sandwich in Ontario for $2.80. And no size of Tim Hortons is $1.50. So the whole exercise just lost me.
We’ll be back tomorrow with a new edition of Covering COVID-19. Sign up here to get it delivered right to your inbox.
[the_ad id=”667878″]
Al Tompkins is senior faculty at Poynter. He can be reached at atompkins@poynter.org or on Twitter, @atompkins.