
 Covering COVID-19 is a daily Poynter briefing of story ideas about the coronavirus and other timely topics for journalists, written by senior faculty Al Tompkins. Sign up here to have it delivered to your inbox every weekday morning.
Covering COVID-19 is a daily Poynter briefing of story ideas about the coronavirus and other timely topics for journalists, written by senior faculty Al Tompkins. Sign up here to have it delivered to your inbox every weekday morning.
Cruise ship companies are thrilled that the Centers for Disease Control and Prevention ended its COVID-19 monitoring program that tracked how many COVID-19 cases were reported ship-by-ship. On Monday, the constantly updated spreadsheet was gone without a trace, replaced with this notice:
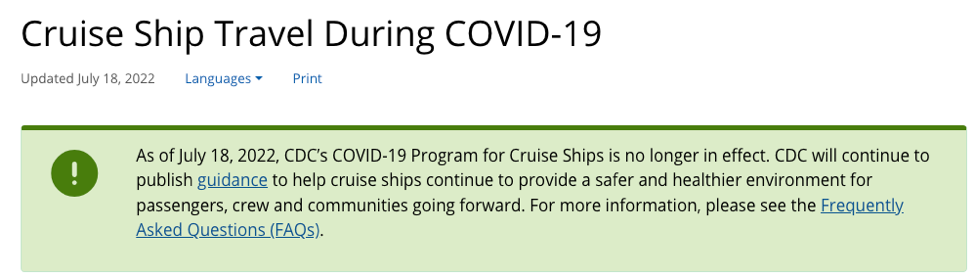
(CDC)
It is hard to make sense of why the CDC would pull back from a detailed monitoring program just as COVID-19 cases are again rising worldwide. (The World Health Organization says cases in Europe have tripled in the last six weeks, and hospitalizations have doubled.)
When the site took down the monitoring page, 93 of the 95 ships reporting to the CDC system had enough COVID-19 cases among passengers and crew to be “under observation” by the CDC. You can see a cached version of the CDC cruise ship monitoring page from July 18 here. Here is a screenshot of that cached dashboard, which shows almost all of the ships reporting COVID-19 data were under observation:
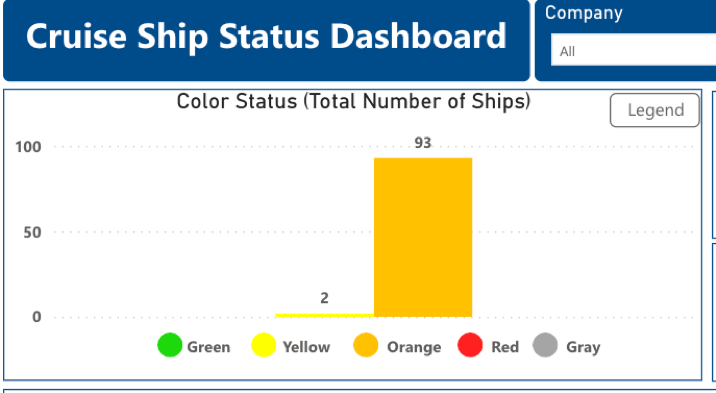
The CDC’s cruise ship status dashboard on July 18, 2022. (CDC)
This is what those colors used to mean:
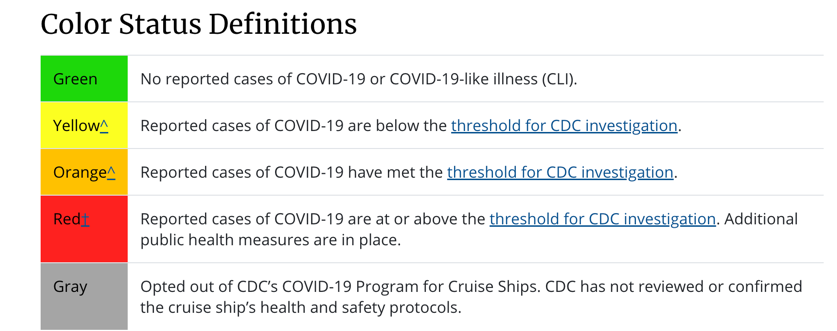
(CDC)
Cruise lines will report COVID-19 data to the CDC, but the CDC won’t pass that information along to you. Instead, the CDC says, passengers “have the option of contacting their cruise line directly regarding outbreaks occurring on board their ship.” In other words, the CDC will still have the data that could allow the public to see the COVID-19 levels on each ship, but it is up to you now to call the cruise line and ask for it.
The CDC website says the now-closed system “depended upon each cruise line having the same COVID-19 screening testing standards, which may now vary among cruise lines.”
CDC spokesperson Kristen Nordlund emailed an explanation to The Washington Post:
CDC has determined that the cruise industry has access to the necessary tools (e.g., cruise-specific recommendations and guidance, vaccinations, testing instruments, treatment modalities, and non-pharmaceutical interventions) to prevent and mitigate COVID-19 on board.
Cruise lines generally require adult passengers to be vaccinated and provide a recent negative COVID-19 test before boarding. Cruise lines have varied requirements for children.
Andy Bloch, who is a master at turning data into charts, posted this. I link to his Twitter post and his exhaustive charts with one caveat: Even the highest COVID-19 numbers on the ships are still not as high as you will find in some counties and countries.
Yesterday, the CDC ended its opt-in “COVID-19 Program for Cruise Ships” that tracked COVID-19 tests and cases. https://t.co/6Zmvug9xdr They updated the data one last time last night. I’ve been extracting the data and decided to publish it here: https://t.co/hWkL5EXOKy pic.twitter.com/SNDYX4v87G
— Andy Bloch (@Andy_Bloch) July 19, 2022
With no pesky COVID-19 data to plant doubts in people’s minds, cruise ship stocks rose fast on Tuesday.
The cruise industry argued that the CDC kept ships under scrutiny that far exceeded any monitoring for concert halls, hotels or convention centers. Earlier this year, the CDC made the reporting program voluntary. But, of course, a key difference is that people don’t live in concert halls for days and go home if they notice sick or reckless people around them.
The CDC’s decision to take down the cruise ship monitoring page also comes just as a new book called “Cabin Fever” by Michael Smith and Jonathan Franklin goes public. It tells the nightmare story of 1,200 passengers and 600 crew stuck on the MS Zaandam when COVID-19 spread through the ship like wildfire during the first weeks of the pandemic’s rage.
WHO warns of COVID hospitalizations rising now, worse to come in a few months
The World Health Organization is warning that the newest variants of omicron are “super infectious” and that COVID-19 hospitalizations, which have doubled across Europe in the last few weeks, will grow worse soon.
Look at these increases from the WHO’s COVID-19 dashboard:

(WHO)
WHO’s Europe director, Dr. Hans Kluge, described COVID-19 as “a nasty and potentially deadly illness” that people should not underestimate. He said super-infectious relatives of the omicron variant were driving new waves of disease across the continent and that repeat infections could potentially lead to long COVID.
“With rising cases, we’re also seeing a rise in hospitalizations, which are only set to increase further in the autumn and winter months,” Kluge said. “This forecast presents a huge challenge to the health workforce in country after country, already under enormous pressure dealing with unrelenting crises since 2020.”
Earlier this week, editors of two British medical journals said the country’s National Health Service has never before had so many parts of the system so close to collapsing.
Kamran Abbasi, of the BMJ and Alastair McLellan of the Health Service Journal wrote in a joint editorial that the U.K. government was failing to address persistent problems worsened by COVID, including ambulances lining up outside hospitals too overloaded to accept new patients.
We barely understand BA.5 and now BA.2.75 is on the way
A coronavirus variant called BA.5 is now the dominant vaccine-escaping COVID-19 variant to infect people in America. But already, the WHO is tracking what could be the next problem: BA.2.75.
The variant has shown up in 15 countries and is on the move. It has been detected in seven U.S. states, including Washington, California, Illinois, New York, North Carolina, Texas and Wisconsin.
The newest variant has gained the unofficial name “Centaurus,” after a Twitter user got the notion that the endless string variants that contain numbers and not a name are not being taken seriously enough.
Keep in mind that every person who gets infected with COVID-19 becomes a host, a potential incubator for the virus to morph again. So, the danger is not just that COVID-19 will make a person sick or cause long-COVID, but that every new case is a potential birthplace for a new threat.
WHO decides tomorrow if monkeypox is a ‘global health emergency’
At last count, 63 countries had reported 9,200 cases of monkeypox, and the number is growing fast. Now the WHO will hear the latest data and decide whether to declare the outbreak a “global health emergency.” That is the highest alarm that the WHO can sound about a health crisis.
The WHO says most infections have been reported in men of young age who have sex with men. Most of the cases are in or near big cities.
The normal initial symptoms of monkeypox include a high fever, swollen lymph nodes and a blistery chickenpox-like rash.
But the report said that in this outbreak, many cases were not presenting with the classically-described clinical picture.
Among the cases who reported at least one symptom, 81 percent presented with a widespread rash on the body, 50 percent presented with fever and 41 percent presented with genital rash.
Monkeypox is usually considered mild and most people recover within a few weeks without treatment. However, the disease is frequently uncomfortable or painful, and can sometimes lead to complications that require close medical follow-up.
The CDC’s latest state-by-state monkeypox case count shows 1,814 cases, which means cases are increasing by a few hundred daily.
The science behind ice cream headaches

Children sitting in a car in Prayagraj, in the northern Indian state of Uttar Pradesh, eat ice cream on Wednesday, April 13, 2022. (AP Photo/Rajesh Kumar Singh)
Ice cream and popsicles definitely are part of the treatment plan to cure summertime overheating. But when it is as hot as it is now, some of us ravage through our frozen treats to keep them from melting … and then the ice cream headache sets in.
There is a quick cure. But first you have to know what causes ice cream headaches.
Ice cream headaches have a couple of fancier names: cold-stimulus headaches or trigeminal headaches. They are “thought to be caused” by the cold treat touching the roof of your mouth and constricting the blood vessels in the palate. I say “thought to be caused” because there is still a bit of mystery behind them.
Here is the clinical explanation of how brain freezes happen from the University of Melbourne:
When a part of the body gets really cold, the blood vessels in that area will tend to constrict. This is called vasoconstriction, and it minimizes the amount of blood that can flow through that area and be cooled down. You might notice your fingers or toes going pale when you’re out in the cold, and this is exactly why!
On the other hand, when your body gets too warm, blood vessels expand to allow more blood to pass through. When the blood vessels near the skin expand, this allows heat to be released and the body to cool down. This is why people can get flushed or red-faced after being in a warm room or exercising.
So, when a really cold substance hits the roof of your mouth or the back of your throat, it causes a rapid change of temperature there. And it just so happens that at this location we find the juncture of two very important blood vessels: the internal carotid artery (which is responsible for supplying blood to the inside of the brain), and the anterior cerebral artery (which travels along the front of your brain and sits right on top of the brain tissue)
When these arteries are hit with the sudden chill of your rapidly consumed ice cream, they constrict very quickly. The body then compensates for this rapid constriction by sending a bunch of blood there to try warm them back up. This causes them to widen. Scientists think it is this contracting and expanding that triggers pain sensors and creates the sensation of pain.
The Cleveland Clinic advises you to bring the temperature in your mouth back to normal to relieve a brain freeze. But a room temperature drink works best; not something too hot or cold that will just cause more blood vessel reaction. The other treatment, Cleveland Clinic says, is to “try pressing your thumb or tongue against the roof of your mouth.”
By the way, people who suffer migraines may be more likely to have ice cream headaches. There is also some evidence that cold stimulus headaches can touch off a migraine.
Johns Hopkins researchers say one of the unknowns about ice cream headaches is why the pain is not felt in the mouth so much as other parts of the head and face:
The pain, through a quirk of our anatomy, is not felt so much in the mouth as it is “referred” to other areas of the face — behind the eyes and nose, in the forehead or elsewhere.
So, you learned another phrase today, “referred pain.”
We’ll be back tomorrow with a new edition of Covering COVID-19. Are you subscribed? Sign up here to get it delivered right to your inbox.





